Retinal detachments are far more frequent than originally thought. Within the next months a article from Nijmegen will be published about retinal detachments and profylactic laser therapy in Wagner syndrome in the large founder mutation family in the Netherlands. The article makes clear that 44.3% of the affected people develope a retinal detachment, predominantly before the age of 15. There is a significant difference between boys and girls. Almost 60% of the boys and just a bit more than 30% of the girls gets a RD. Girls however develop more bilateral detachments. Half of the girls with RD face bilateral detachment, whereas only 10% of the boys with RD develops a RD in the fellow eye.
In approximately one third of the cases the macula is off. That is the part of the retina that is used for reading. In these cases surgery will not restore vision as it was. Although surgical techniques have improved enormously, the functional outcome for younger patients (born after 1962) is less than 0.1. In another 20% de visual acuity after surgery is between 0.2 and 0.4.
Since 1973, when laser therapy became available, 63 eyes were lasered in the Nijmegen Medical Centre to prevent retinal detachment.
The upcoming publication makes clear that laser is not effective in Versican-Wagners. On the contrary, in young patients it can cause RD: in almost 40% of the retinal detachments in the group born after 1962, RD developed within 5 weeks after laser therapy.
cataract
Presenile cataract (progressive loss of transparency of the ocular lens) is a common finding and a common cause of decline in visual acuity over time. The types of cataract vary. Small spherical opacities and posterior sub-capsular cataract affected almost half of the Swiss family. In the Dutch families, cataract types included moderate cortical cataract, anterior and posterior cortical cataract, and posterior sub-capsular cataract. Nuclear cataract without any posterior sub-capsular opacity was described in a British family. In a Japanese family, approximately 50% of the family members underwent cataract surgery. In the French family, cataract affected 55% of the people.
myopia
Myopic refractive error (nearsightedness) results from axial myopia (a developmental mismatch of the refractive power and length of the globe) and/or index myopia (a change in the refractive index of the progressively cataractous lens). Axial myopia is common, although severity varies. In the family reported by Wagner, a lot of members had mild myopia and only a few had moderate to severe myopia. In contrast, in the Dutch family a lot of members had high myopia with astigmatism.
symptoms

With all of these symptoms it is obvious that the visual acuity is not normal.
At this moment there is no overview of visual acuity in the various pedigrees.
vitreoretinopathies
Apart from Wagner there are several other hereditary disorders that affect retina and / or vitreous. Below you will find these disorders. We only mention the symptoms that differ from Wagner.
erosive vitreoretinopathy
5q13.4
-
-erosion of retinal pigment epithelium
-
-vitreous syneresis
stickler syndrome
type 1 (COL2A1)
12q13.11
and
marshal syndrome
stickler type 2
1p21.1
- abnormal vitreous
-
-retinal detachment (more dan Wagner)
-
-systemic abnormalities in facial and skeletal structure, hearing problems, arthritis
knobloch syndrome
21q22
-
-nastygmus
-
-cataract with lensluxation
-
-vitreous degeneration, type unknown
-
-macular degeneration
-
-retinal detachment (more dan Wagner)
-
-occipital enchepalocele or scalp/hair defect
enhanced s-cone syndrome
(wo Goldmann-Favre)
15q22
-
-normal vitreous, except maybe with Goldmann-Favre
-
-no cataract
-
-cystoid changes
-
-ERG: enhanced s-cone
autosomal dominant vitreoretinochoroido-pathy
11q13
-
-normal vitreous
-
-no cataract
-
-optic nerve may have neovascularisation
-
-macular edema
-
-few retinal detachments
-
-ERG: reduction en depressed Arden ratio
snowflake vitreoretinal degeneration
2q36
-
-corneal guttata
-
-flat appearance optic nerve, absent cup, waxy pallor
-
-minute inner retinal crystals
-
-ERG: reduced dark-adaptation, b-wave reduction
with courtesy of
AO Edwards,
Mayo Clinic,
Clinical features of the congenital vitreoretinopathies, 2008
wrong diagnoses
For a long time Stickler and Wagner were confused by doctors. But since the genetic cause has been established, that is no longer the case.
Ocular features in Stickler and Wagner are more or less the same, but people with Stickler syndrome also is associated with cleft palate, joint and bone problems and hearing loss. Wagner is ocular only.
And than sometimes doctors say Wegener disease and patients hear Wagner disease
Wegener granulomatosis is an auto-immune disease that can have devastating effects. For more information, click here.
Not in every pedigree the same things are measured. Therefore it is not easy to establish what the symptoms of Wagner syndrome are. Or sometimes data are no longer available. So if some symptoms are not mentioned in a certain pedigree it doesn’t mean it wasn’t there. It is simply not measured or not mentioned in the article.
vitreous
Wagner syndrome is one of the connective tissue disorders that is affecting the collagen. The most distinct issue is the vitreous. Normally that is a jelly-like substance. In people with Wagner syndrome the vitreous is ‘optically empty’ with floating fibrils and / or strands.
The hallmark is a circumferential vitreous condensation. It is seen as a shiny white line on the retina near the equator. In some patients this line is visible as a clear, white band, whereas in others it can only be found with difficulty as a subtle, linear refraction. This line is found to be the origin of a forward extending preretinal membrane, of which the line itself can be seen as a local ridge near the retina.
This unusual vitreous can be observed already in very young children. There is no difference between male or female.
This vitreous degeneration, which is assumed to be the primary pathology, leads to a number of secondary changes, including cataract before the age of 40 (‘presenile’), degeneration and atrophy of the retina and the underlying retinal pigment epithelium (RPE) and choroid, and retinal detachment.
retina
Nonspecific reactive changes of the retinal pigment epithelium and overlying retina (pigment condensation, vascular sheathing, pigmented lattice degeneration, and later chorioretinal atrophy in the retinal periphery) occur. Affected individuals may experience nyctalopia (night blindness) and visual field constriction that are not as severe as those seen in retinitis pigmentosa. Nyctalopia (night blindness) may or may not progress. In some cases the chorioretinal atrophy is so severe that it resembles choroideremia.
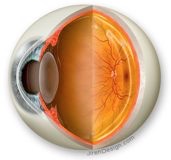
fig. the eye, cross section
right the retina (macula, papil),
left cornea, iris and lens
page last modified Jul 29th 2014
occasional ocular features
The following features have been reported rarely. Some may not be part of Wagner syndrome but rather occur coincidentally.
Spherophakia, a spherical deformation of the ocular lens, has been observed sporadically in persons with VCAN-related vitreoretinopathy (Swiss family)
Cataract can induce a change of the refractive index of the lens nucleus, further attenuating the myopic refractive error (index myopia).
Posterior vitreous detachment (PVD), detachment of the posterior vitreous membrane from the retinal surface, is caused by shrinkage of the vitreous body and the pathological vitreoretinal interface. In contrast to the usual age-related PVD, the PVD in VCAN-related vitreoretinopathy initially affects the peripheral rather than the central posterior vitreous.
Ectopic fovea, manifesting as an increased angle kappa (the angle between the visual axis and the pupillary axis), has occasionally been reported (Swiss, Japanese, British family)
Phthisis bulbi (painful shrinking of the ocular globe as a result of loss of intraocular pressure) can occur and may require enucleation of the eye. Retinal detachment that has not been repaired successfully and retinal detachment associated with proliferative retinal vitreoretinopathy (PVR) are risk factors for phthisis bulbi. The decrease in intraocular pressure is caused by decreased aqueous production by the ciliary body epithelium, which becomes compromised by the pathologic vitreoretinal membranes because of the primary vitreous changes, the PVR, or both.
Synchysis scintillans (bilateral accumulation of cholesterol crystals in the vitreous, which may or may not be associated with recurrent vitreous hemorrhage), may or may not occur with increased frequency in VCAN-related vitreoretinopathy, as it was only observed in a few older affected individuals.
Optic atrophy was found in only a few of the older individuals from the Swiss family. These individuals had advanced chorioretinal atrophy, suggesting that optic atrophy is secondary to the massive loss in retinal ganglion cells.
Glaucoma may not be a common feature of Wagner syndrome, as only a few individuals with VCAN-related vitreoretinopathy have been reported with glaucoma, none of them having primary open-angle glaucoma (one had congenital glaucoma, two had chronic angle-closure glaucoma, and three had neovascular glaucoma).
In the Swiss family (Graemiger 1995) more than half of the eyes of the studied population had an abnormal anterior chamber angle (dysgenesis or narrow)
In the Dutch family B (Jansen 1966) there is a question of elevated intraocular pressure without glaucomatous damage: average IOP was 21,32, n=24, range 11-39 mmHg, sd 4,97, age 10-75). Almost everybody over 30 had an IOP > 22 mmHg.
systemic findings
To date, no systemic abnormalities associated with VCAN-related vitreoretinopathy have been reported, and consequently VCAN-related vitreoretinopathy is considered an isolated vitreoretinal degeneration.
(with courtesy of Barbara Kloeckener-Gruissem et al in gene reviews)
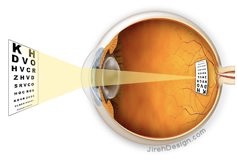
fig. The eye has to have enough total refractive power (cornea, lens, vitreous) to get the image on the retina
Wagner syndrome
Illustrations: with courtesy of www.jirehdesign.com


The full-field electroretinogram (ERG) becomes attenuated. Typically both the amplitudes of the a-waves (response of the photoreceptor layer) and the b-waves (response of the bipolar cell layer) are reduced. The rod and cone systems (as measured by the scotopic and photopic response, respectively) are affected to varying degrees but in a family-specific manner, as demonstrated by the Swiss family originally reported by Wagner, the Japanese family, and the British family. No ERG measurements were reported from the French and only few of the Dutch family.
Abnormal retinal vessels or poor vascularization of the peripheral retina were found in several families (Swiss, Dutch).
image. retinal detachment
(♀12 yr, os)
The white circular line is a special feature in the Dutch family
described by Jansen (1966)
Click on the drawing to enlarge
© vl nas
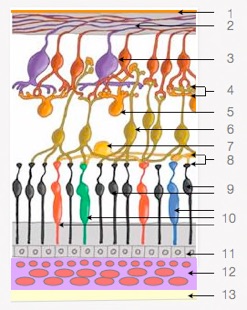
image: retina, choroid, sclera
1 internal limiting membrane
2 nerve fiber layer
3 ganglion cells
4 inner plexiform layer
5 amacrine cells
6 bipolaire cells
7 horizontal cells
8 outer plexiform layer
9 rods
10 cones (blue, green en red)
11 pigment epithelium
12 choroid
13 sclera
links to websites about other vitreoretinopathies
stickler
fevr
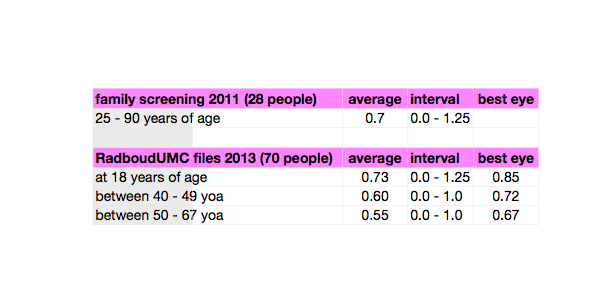
visual impairment
Most people with Wagner syndrome experience a decrease in vision, but most of them wil not get severely visually impaired or blind. It seems that most people do need more contrast / light when they age.
In Radboud University Medical Centre Nijmegen (the Netherllands) there are almost a hundred patients known with this disease. There visual acuity in relation to their age is: